
<1>In 1886 at a meeting of the Pathological Society of London, Dr. W. Bruce Clarke told his audience about one of his young patients, “Samuel W–.” After an apparently normal infancy, Samuel began to “eat voraciously” at nine months of age. He grew “hair [. . . ] upon the pubes,” and his “penis rapidly acquired the character of a man’s, and was often [. . . ] erect.” He experienced “prodigious” growth. By the time Clarke saw him at age three years, three months, he was “a well-developed muscular lad, looking about twelve or thirteen years of age,” but “No seminal emissions have ever been noticed.”(2) He had little body hair but a “Well-marked Pomum Adami,” and “he laughs with a peculiar hoarse croak.” Aside from surgery to correct bowed tibiae,(3) Clarke mentioned no other medical treatment (358-9).
<2>The subject of this essay is very early puberty, that is, puberty appearing at age three to six or seven years of age, a phenomenon I attempt to explore and analyze at the intersection of medicine, gender, and culture. In examining early puberty as seen through the eyes of nineteenth-century doctors, I will argue that these doctors’ ideas about the nature of early puberty were shaped by gender – their own and that of the child-patients they examined. They saw pubescent girls and boys through the lenses of Victorian sexual identity and expectations, as well as those of race, class, and nation. This essay locates early puberty in the discourse of disability. This may, at first glance, seem strange, for precocious puberty would seem more a case of early ability rather than disability. But early puberty can also be understood as deviance, as straying from norms of bodily development. In the phenomena of early puberty doctors found amazement, desire, and dread.
<3>This paper is based on the published writings of nineteenth-century medical men. This means, in the first instance, that this was public discourse. It was also professional discourse, primarily intended by the authors and the journals for the information of other medical practitioners. These publications, primarily articles and reports, in most cases provided brief accounts of individual medical cases, their origin, treatment (if any), and outcomes. Occasionally a medical writer took on a more extended task, for example, describing a number of cases and using them to sum up the present state of knowledge, to argue for a particular interpretation of causation, or to recommend treatment. My purpose here is to use these medical writings to explore the gender relationships that existed between doctors—all male—and the bodies and persons of their patients, male and female.
<4>A note on usage: I will use the term “pubescent child” to refer to the subject of the medical case whom the doctors described as undergoing precocious puberty, to avoid the clumsy locution of “a child undergoing puberty at an abnormally young age.”
<5>There was general medical agreement about the normal signs of puberty in both sexes. Signs of female puberty included breast development, pubic and axial (underarm) hair, the enlargement of the buttocks and pudendum, and, of course, menstruation. In males, the signs included the growth of pubic, axial, and sometimes facial hair; muscular development; erections; nocturnal emissions; and a low or hoarse voice. The normal age for the appearance of such signs was thought to be age twelve to fourteen, with some developing earlier, others later.(4) Across the nineteenth century, British doctors reported cases of children brought to their attention who were displaying the marks of puberty long before the normal range.
I. Precocious Puberty in Females
<6>Early reproductive maturation in a female child typically came to a medical man’s attention when her mother discovered that the child was bleeding from the vagina, and given the child’s age, was certain that the bleeding was pathological. Five-year-old Jane Jones, for example, came under Thomas Peacock’s notice “when,” he reported, “I was consulted by her mother in consequence of a discharge bearing every resemblance to the catamenia” (548). He examined the blood as to its quality and the regularity of its appearance. Dr. A. Cookson saw little Charlotte Maver at age four and pronounced hers a “most extraordinary” case. She began menstruating irregularly at age three and one-half. Later her periods came “regularly every four or five weeks” (Cookson 117). When the London surgeon Astley Cooper examined her at age four, he found the blood “exactly resembled that of most women, except that it was of a rather darker colour” (204).(5) He examined her again at age six, and “she has continued to menstruate” (Cooper 205). Three-year-old Jane Jones’s menstrual cycle appeared “regularly” from the first (Peacock 548).
<7>When the medical man examined such a bleeding female child, he typically looked for other signs of early physical maturation. Cookson described his patient’s breasts as “uncommonly large and protuberant” (118). Astley Cooper described Charlotte’s physical development: “The breasts are very full, and as large as most young women’s of twenty years of age.” At age six, she was only one inch shorter than her ten-year-old sister (205, 206). At age three, Jane Jones’s breasts “were observed [by her mother] to be unusually large,” and by age seven, Dr. Peacock could affirm, “Her breasts exceed the usual size of these organs in unmarried adults” (548). As for other physical signs of puberty, Cookson found his patient’s “nates [buttocks] and shoulders [. . . ] as large and as broad as those of a grown-up woman.” He added that “the [. . . ] pudenda [are] as prominent as those of a girl of sixteen,” and the “mons veneris and labia” were “furnished with a downy kind of hair” (118). “Mary D.” began menstruating at age three years and six months. Dr. Smart saw her a year later, and he described her physically as “wonderfully like that of an adult female of short stature,” with “breasts large and prominent, [. . . ] nipples [. . . ] well developed,” and “hair on the pubes [. . . ] light brown” (132).
<8>Doctors looked, too, for behavioral signs of a girl’s stage of development and particularly for any social effects of early sexual maturation. They expected that females who had undergone normal puberty would display marked modesty, presumably because they were self-conscious about changes in their bodies. When Astley Cooper first saw Charlotte, he reported that “her countenance [. . . ] is childish,” and she “does not seem to have any sexual feelings, or an uncommon degree of modesty” (205). By age six, Charlotte displayed “a degree of modesty not formerly noticed.” Her mother told Cooper that she “does not now like to walk in the streets, because some boys have teazed [sic] her about her appearance” (205). Dr. Cookson’s patient did “not [. . .] exhibit any particular marks of attachment to the other sex,” and “Mary D—…gave no positive indication of sexual propensities” (Cookson 118; Smart 132). Another pubescent child, Jane Jones, was, according to her mother, “averse to any allusion being made to her peculiarity by any of her own sex, and displays a degree of modesty in her conduct towards males unusual in children of her age” (Peacock 549). With normal sexual maturation came interest in the opposite sex. Such change would, at the normal age of puberty, typically and respectably be accompanied by a new modesty and decorum in a female’s relationship with males. Jane’s mother thought she saw such modesty, but the doctor, Thomas Peacock, seemed to find it reassuring that he did not: he found Jane was “in her amusements [. . .] as childish as the other children in the school” (549).
<9>Issues of sexual attraction and desire led doctors back to biology. Some doctors speculated as to “how far it is possible for the female to become impregnated at the early period at which [. . .] the catamenia appeared” (Peacock 550). Cookson raised, as “a matter of curious speculation, whether this child [Charlotte] could be impregnated, conceive, and produce her kind. I am inclined to think in the affirmative” (118). Such propositions with respect to British children are relatively rare. Discussing foreign cases of early puberty, however, led to implied cultural comparisons. John Forbes, for example, reported on an American case. Dr. Justus Ledseau of New Orleans wrote to Forbes about five-year-old “Martha H.,” who “came from “a white family in low circumstances” (qtd. in Forbes 9). He reported that “The dimensions of the pelvis are, in my opinion, such as to enable her to bear children when eight years old, and very likely sooner” (qtd. in Forbes 9).(6) Peacock pointed to an eighteenth-century Parisian case “of a girl who menstruated at 2” and was “delivered of a dead child at 8 years and 10 months” (550). Roberton, in commenting on puberty at age ten or eleven in Mediterranean and South Asian regions, observed that puberty in those areas, at whatever age, was accompanied by “early marriage and early intercourse” which led to “early fecundity” (1).(7) Precocious female puberty led doctors, indirectly or directly, to child sexuality and reproduction, most comfortably viewed at a social or geographic distance.
II. Precocious Puberty in Males
<10>Early puberty in male children brought them to medical attention when they exhibited physical signs that parents found worrisome. The eminent surgeon John Flint South presented the case of John Sparrow (b. 1818) to his colleagues in the Medical and Chirurgical Society of London in 1822. The boy was the son of “labouring people”; the father was “a thin but healthy rustic,” and the mother “a dark little woman” (South 76). South relied on the recollections of Sparrow’s mother for information about his physical and mental development up to age four. Of particular interest was the baby’s hair. At birth he was “completely covered with hair,” much, one might surmise, like a baby animal, rather than a human newborn (South 76). When he was four months old the “hair on the pubes began to grow very quickly” (South 77). The dark hair on his head was, after weaning, replaced by “light curling hair” (South 78). The boy’s mother observed that “His voice[. . .] was always gruff” (South 79).
<11>His remarkable growth included the genitals: South, still presumably reporting on the mother’s observations, reported that the baby’s “penis increased in size, particularly the glans, so that it extended beyond the prepuce” and at fifteen months “was entirely exposed” (77). The mother became concerned when, after he was weaned at age fifteen months, “his linen was stained two or three times in the week” (South 78). When she noticed “his crying out whenever it occurred, as if hurt, and the circumstance of his being faint and pallid on the next morning,” she began to watch the child more closely and (as the doctor obliquely put it), she “ascertained the real cause” — nocturnal emissions — “alarming her very much” (South 78).
<12>South examined the four-year-old boy’s physical and muscular development: “When his clothes are stripped off, the trunk presents the appearance of that of an adult, except that he is not so large across the shoulders as he is round the pelvis.” Moreover, “He has a large and ample chest, on which the pectorals are prominent” (80). His “thighs are large and muscular, but out of proportion.” South judged that “the posterior view of the trunk [of the four-year-old][. . .] presents, next to the parts of generation, the most remarkable appearance” (South 81). South was clearly amazed: “The lumbar mass of muscles is enormous, and the trapezius” and “the latissimus dorsi, are not a whit behind them” (81). Physical power accompanied this boy’s growth. He showed his “very great strength” by “lifting a half-hundred weight with one hand, with great ease” (South 81). South also, of course, examined the genitals and confirmed what the mother had reported: “The penis, scrotum, and testicles are as large as those of an adult: the prepuce being always drawn back, or perhaps, it may be said, not existing at all; the glans penis is constantly uncovered” (81).
<13>Dr. James Devon, in an early twentieth-century case, followed a similar path of reporting on the remarkable development of boys in early puberty as to facial hair, large genitals, pubic hair, and voice (340-1). Perhaps Dr. Guthrie’s report offers the best capsule description of a precociously developed boy: “Henry M.,” he reported, presented “a striking resemblance to a burly brewer’s drayman in miniature” (748).
<14>From the mid-Victorian period, photographs entered the arsenal of Victorian medical communication, and a few pictures of pubescent boys appeared in the medical literature. The photographs from Dr. Harry Campbell’s 1896 report shown below are those of a six-year-old boy.(8)
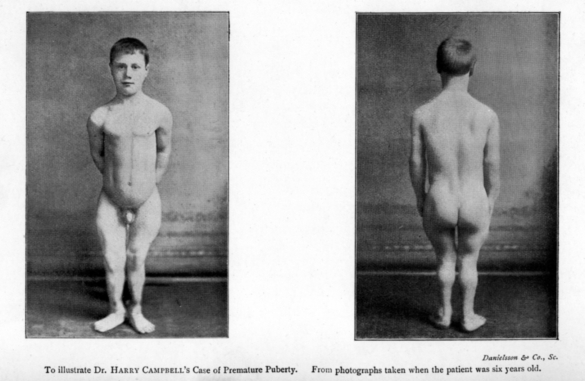
These photographs verified for Campbell’s audience and readers the unusual physical development of this child.(9 Later, with the new technology of the skiagram (early x-ray), Devon could offer images of the early maturation of joints in his early pubescent subject (339).
<15>As with their female subjects, doctors looked for personality changes or abnormalities in these pubescent boys. John Flint South recounted what young Sparrow’s mother told him: the child is “very passionate, but his rage is soon over, and he is very anxious to be reconciled, if he thinks he has affronted his mother.” He was like other children in that “When vexed he cries bitterly” (79). When South examined the little boy, he found the four-year-old boy “at first shy” but cooperative, “remarkably inquisitive” and possessed of a good memory, and easily amused (82, 83). The child seemed, in other words, a normal little boy, despite his unusual physical development.
<16>One mark of maturity in Victorian males was self-control, and medical men examined these boys to see if self-discipline accompanied their extraordinary physical development. With respect to impulse control, young Sparrow was more little boy that adolescent, but other doctors found notable differences. Dr. Clarke found that his patient lacked discipline in his eating habits: in 1886 he specially noted that the one-year-old boy “suddenly [. . .] began to eat voraciously, his appetite being larger than that of a full-grown man. He bolted his food and nothing appeared to satisfy him” (358). Clarke seems to have found this conduct repellent.
<17>Hugh Lett noted the lack of self-control in the unnamed boy whose case and photograph he presented to the Society for the Study of Diseases in Children early in the twentieth century. This child developed all signs of puberty between the ages of two and four years—pubic hair, genital development, erections, nocturnal emissions, deep voice, and “great physical strength” (200). “His appetite was voracious,” Lett said (201). When it came to intelligence, “Intellectually he was bright, but he had a terrible temper" (201). Here was a child whose “terrible temper” could not be blamed on any physiological problem that Lett could find. And his undisciplined temper was matched by his excessive appetite. R. P. Rowlands examined a “Boy, aet. 2,” who had multiple signs of puberty including “large external genitals” and a “faint moustache.” Like Lett, this doctor described his pubescent patient as “of vicious temper” (256).
<18>As with their female cases, doctors sometimes raised the question of sexuality in these pubescent boys. Their precocious erections and apparent ejaculations strongly suggested sexual maturation. Dr. Harry Campbell had a patient who “manifested considerable sexual excitement” before the age of two” (214). Dr. Devon’s ten-year-old patient found himself accused of sexual misconduct, but he denied “being in the habit of doing ‘nasty things’ to girls.” The boy did admit that when he was eight-and-one-half he was taken to a park by an older girl, where “she lay down and showed him what to do” (342).(10) Peacock reported on early male sexuality in a French case—“a woman who stated herself to have been impregnated by a boy of ten years old” (550). Here again, the foreign case offers the extreme expression of precocious sexual development.
III. Causation and Treatment
<19>Early nineteenth-century accounts of early puberty included little in the way of speculation on the causes of precocious development. Reports of family background (e.g., father’s occupation, parents’ health), which were typical of medical case reports in this period, may have implied causation, but doctors made no explicit connections. Dr. T. Wood, for example, noted without comment that the father of a boy with early puberty “is in a lunatic asylum” (377). One early theorist suggested that precocious puberty began “in utero,” but J. F. South “was not satisfied” (85).
<20>Heat, both physical and metaphorical, was a common early Victorian hypothesis for the cause of early puberty. Dr. Peacock speculated that early puberty in a young continental boy resulted from “his having mixed in the turmoil of the [French] revolution,” presumably because it was an exciting time (550).(11) He noted that children subject to the heat of the factory or overcrowded urban conditions could undergo puberty several years ahead of what was normal. The “heated atmosphere to which they are exposed must make their constitutions nearly allied to those of the natives of warmer climates” (Peacock 550). While at mid-century, Dr. John Roberton argued vociferously against the notion, held by other doctors, of warm climates being a cause of early puberty,(12) in the late nineteenth century at least one doctor continued to speculate on the relationship between environmental conditions and the onset of puberty.(13)
<21>In the early twentieth century doctors explicitly included heredity among possible causes of precocious puberty. James Devon’s case study of a Glasgow boy included a survey of the history of the boy’s siblings’ ages at puberty (342). Following Dr. Hugh Lett’s paper at a 1906 meeting of the Society for the Study of Diseases in Children, his audience seemed especially interested in discussing causation. Dr. Shuttleworth specifically asked about “any family history which [could] throw any light” on a similar case, and suggested that the father’s illness “at the time of the conception of the child” might be related to the child’s condition (Lett 202). Dr. F. Parkes Weber suggested that precocious puberty reflected “reversion to a lower type of animal,” a sort of evolutionary throw-back (Lett 202). Others made the case for tumors in the ovaries, testes, or pineal gland as the likely cause of premature puberty (Lett 202, 203).(14)
<22>The cases I have examined involved children as young as two years of age, more often age four or five. Sometimes doctors followed these cases for several years. In most cases doctors made no mention of treatment, but occasionally cold baths were recommended for pubescent boys (South 78). When tumors became suspect in the pathology of early puberty, their removal, doctors reported, reversed the precocious development.(15)
IV. The Meaning of Early Puberty
<23>Precocity, at a minimum, implied deviation from some norm. “Thus,” wrote R. L. Langdon-Down, “primitive races are said to be precocious as compared to civilized races.” He went on to say that “some race standard of either maturation or development is assumed” (744). In short, precocity distinguished the “primitive” and the “civilized.” The existence of these primarily British children with precocious puberty offered nineteenth-century medical men opportunities for comparisons and distinctions that reveal the meaning of the sexual precocity they had examined.
<24>In my analysis of medical accounts of pubescent children, I have found three broad themes in the discourse: the sense of “wonder,” with the related notions of the exotic and the scandalous, and the responses of desire and threat. The notion of wonder (including amazement) suggests the importance of the gaze to both attraction and repulsion. These lead us to consider the relationship between the spectacle and the showman.
A. Wonder
<25>Early on, John Flint South insisted that his patient’s “case is rare and curious” with “the most remarkable appearance” (85, 81). In the 1880s, doctors were still using that kind of language. In The Lancet in 1882, Woods reported on "An extraordinary case of early puberty in a boy," and Clarke described his patient’s growth as “prodigious" (Woods 377; Clarke 358). These examples illustrate the common thread in nearly all of these medical reports—the use of such words as “remarkable,” “unique,” “wonderful,” “strange,” or “extraordinary” to refer to these cases of early puberty. Such language is peculiar because, for most of the century, doctors’ case reports seem intended to contribute to a pool of shared experience about disease and treatment, with the hope that one doctor’s observations might be helpful to another. This language of the unique harks back to an earlier age, when physical deformities were thought to be signs or portents or sources of amazement and wonder—and perhaps amusement. But this language of amazement also relates to the carnivals and side-shows (and even quack medicine shows) of the nineteenth century, where people with physical anomalies were subjects of carnival display or profit-seeking exhibitions.(16)
<26>Despite the scientific nature of the publication venue and the medico-scientific qualifications and aspirations of these authors, they present their cases in a manner to provoke amazement and wonder. Very much like the freak shows and circuses of popular entertainment explored by Rosemarie Garland-Thompson and her colleagues, these medical cases focus on the spectacle of visible physical difference. The philosopher Elizabeth Grosz argues that the importance of the deviant body to the viewer comes from the fact that such bodies “imperil [. . .] the very categories we rely on to classify humans” (Thomson 57). In the case of pubescent children, their evident display of adult physical characteristics and capacities excluded them from the (normal) category of “child,” while their chronological age, short stature, and psychological immaturity excluded them from any possible standing as adults.
<27>The pubescent child, unlike the bearded lady and the two-headed goat, did not provide entertainment to medical readers or a thrill-seeking public. But like the carnival’s displays, these children were the objects of professional exploitation. Doctors used the occasion of the children’s deviant physiologies to get their own names before the professional reading public. Hence, linked to the scientific purposes of medical publication were some of the same impulses that brought fame and fortune to the Barnum and Bailey entrepreneurs.(17) For the doctors, published cases of precocious puberty could have been attention-getting devices and, they may have hoped, the avenue to notice and enhanced income.(18)
<28>Closely related to the reaction of amazement or
wonder is the identification of the exotic.
Most medical observers of pubescent children remark on their
“darkness.” South mentioned the “dark” blood. Peacock noted the
“dark areola” of his patient’s breasts (549). South also found
“thick dark curling hair” growing on his patient; he later
emphasized the “particularly [. . .] black hair” (South 81, 76).
He reported that the “hair on the pubes began to grow very
quickly and black,” and at fifteen months the “pubes were then
completely covered with black curling hair” (77).
<29>Such emphasis on the dark and hairy features of these children might be explained by reference to their inherited family coloration, but in almost no case did doctors attribute this dark hair growth or dark nipples to family resemblances. Like the linkage of puberty and excessive heat – whether in the factory districts or the tropics — the often unspoken linkage here between heat, physical maturation, dark features, and early sexuality points directly to the sort of social, racial, and ethnic stereotyping that characterized British notions of the “lower orders,” foreigners, from France to Africa and India, and the “primitive.” Such associations suggest connections to the “less civilized” peoples of the laboring districts and the Empire or the throwbacks to an earlier stage of human evolution. In doctors’ minds these pubescent children were in some way alien, exotic, deviant, uncivilized, and un-English. These early pubescent British children thus shared an identity with the Other—the denizens of the overheated world of the factory, the sturdy working class, and foreign southern climates.
B. Desire
<30>Doctors report in detail their
examinations of pubescent children, and they are revealing.
Astley Cooper described four-year-old Charlotte Mawer to his
colleagues at the Medico-Chirurgical Society of London as “quite
a little woman in her appearance” (205). Cooper’s tone is
distinctly approving, as was Cookson’s when he said his patient
“is a strong-built womanly kind of child” (118).(19)
Sometimes doctors’ language suggested that they found these
girls physically attractive. Peacock described his female
patient, Jane Jones, now age seven, in positive terms, observing
“her limbs full and rounded.” Of her breasts he reported,
with apparent enthusiasm (and clearly from personal
examination), that “the gland is large and firm.” Peacock
noted that Jane’s breasts “possess the erected nipple, and in
some degree the dark areola, of the pregnant state,” and that
compared with her sister, age fourteen, Jane was “much more
womanly in form” (548, 549). Similarly, Dr. Ledseau described
his American female patient as having “mammae perfectly formed,”
and, he added, “she is what may be termed handsome” (Forbes 9).
<31>R. B. Smart echoed this enthusiasm in the 1850's when he described his patient Mary D., age six, as having a “bust full and womanly; the breasts large and prominent, with the characteristic glandular feel on manipulation.” He continued: “Her general appearance is wonderfully like that of an adult female of short stature” (Smart 132). Smart expressed wonder, perhaps even approval of, her appearance.
<32>The elision of girl and “little” woman reveals, once again, how easily Victorian men could put adult woman on a footing not far from that of children—the ease with which the identity of the adult woman could be incorporated into the pubescent child. It also suggests, more darkly, the element of adult male desire for the innocent female child. This desire can be seen elsewhere: in the sometimes controversial girl-photographs by Charles Dodgson (a.k.a. Lewis Carroll) and in the infamous reports of the sale of virgin (often pre-pubescent) girls from impoverished families to wealthy roués uncovered by the journalist William T. Stead and reported in his newspaper, the Pall Mall Gazette and then in his pamphlet, The Maiden Tribute of Modern Babylon.(20) Medical men faced the issue most candidly when looking abroad. Dr. McLeod, for example, reported on the physical consequences resulting to “an immature girl from sexual intercourse with a mature male,” mentioning, among others, an eleven-year-old girl and a thirty-five-year-old man, drawing his illustrations from trials in the Calcutta High Court (278).(21) The pubescent British girl was safely mirrored in the “oriental Other.”
C. Danger and Dread
<33>Doctors generally agreed, for much of the century, that precocity, whether physical or mental, was at best risky, sometimes positively dangerous. Precocity was disorderly, a violation of the natural process of development.(22) Puberty, too, whether early or normal, could be a hazardous time of a child’s life. Clouston’s 1880 description of adolescence explained why it was a period of risk and what measures, particularly dietary, could be taken to minimize potential problems.(23)
<34>Most doctors had limited contact with these pubescent children. Nevertheless, some doctors inferred, from the early and rapid development of sexual maturity, equally early processes of aging and death. Dr. Guthrie observed one three-year-old girl who looked like “a little old woman past the climacteric period [i.e., post-menopausal]” (748).(24) Cookson expressed, without specifics, apprehension that his female patient “will not survive many years (118).” Guthrie concluded that “In most cases precocious development is soon followed by rapid degeneration. The condition is one of progeria or premature senility. They die ‘enfeebled old dotards at five’” (749). A whole, brief life might be foretold in precocious puberty.
<35>It is not surprising, then, that Victorian medical men found the potential for trouble and even danger in abnormally early puberty. Dr. Cookson found “no evidence” of his female patient’s “attachment to the other sex.” But, he added, I “have thought it right to caution the mother on this head” (118). Cookson may have framed the issue in terms of the girl’s “attachment”—but implicit in his warning is the danger from the desiring male. Sexual desire was a problem in boys, too. Dr. Harry Campbell’s sexually excited two-year-old male patient showed these symptoms until the age of seven, “since which time it has ceased to trouble” (214). Such early visible sexuality clearly troubled some: perhaps the child, perhaps the family, perhaps the doctor, perhaps all of them.
<36>Danger was not limited to the pubescent children themselves, but included their peers. John Flint South found that his boy-patient was “like a strong muscular man [. . .] of very great strength,” But “though his body,” South noted, “is so completely evolved,” he “still acts from the impulse of the moment” (82). If “he be opposed in the most trivial thing, he will throw himself into a violent passion, chastise the offender, if it be in his power, or, if not, vent his indignation in a flood of tears” (South 83). The boy’s extraordinary body was wedded to an immature, undisciplined, and emotional temperament. Given the boy’s extraordinary size and strength, South noted, he was a dominant figure among his peers, and “he uses his fist with good effect” to get what he wants from the other children (79).
<37>A more extreme case of child-on-child violence came to medical attention when surgeon James Devon was called on to examine a ten-year-old pubescent boy who was in jail.(25) This boy, weighing in at 120 pounds, had earlier been known for “striking” smaller boys who teased him about his appearance. But he was in jail “await[ing] trial on a charge of “attempting to ravish a girl” (Devon 339). Predictably, the family, teacher, and priest denied the charges. The doctor distanced himself from the case by noting the “respectability” of the family (although not their gentility) and by implying that the boy’s behavior could be blamed on an older, promiscuous, and presumably working-class girl (Devon 341).
<38>Buried in J. F. South’s account of the “muscular” boy were the signs of a potential physical threat to adults. With “great ease,” South noted, the boy “will drag an adult about on his rocking-horse, without much exertion” (81-2). The four-year-old boy could potentially challenge an adult. In 1882, Dr. Woods saw a case of early male puberty in a child he examined at the age of six, but whom he had known from birth (377).(26) The boy was committed to an “industrial school” because he was so “wild and mischievous [. . . ]. It required three policemen to take him to the workhouse” and there “he smashed a bedstead into atoms, kicked plaster off the walls, cursed and swore in most fearful manners,” at which point he was taken to the police station (Woods 377).(27)
<39>While the females in early puberty were described as “childish” or “modest,” such violent conduct of pubescent boys could evoke fear. These boys’ conduct, too, was childish, but given their size and strength, their undisciplined behavior (however boyish) posed a threat to adults, including the doctors. Early female puberty only underscored the acceptable female characteristics of modesty and propriety, but early male puberty posed multiple threats. The disorderliness of little boys, manageable with normal physical development, became a positive threat with early puberty. The dangers posed by their visible sexuality and strength could most comfortably be discussed when identified with the “lower orders” or foreign populations.
<40>Later in the century we can see hints of change in some doctors’ responses to boys undergoing early puberty. When some doctors saw that same muscularity at the end of the century, their vision of appropriate masculinity had changed. From the disciplined manly ideal of the early century, described by such scholars as James Eli Adams, another model had arisen.(28) Now the occasional doctor was describing early-pubescent males as boys of “the muscular or infant Hercules type,” underscoring the massive size and strength of the boy’s physique (Guthrie 749).(29) The “muscular Christian” ideal become, later in the century, a more secular (indeed pagan) muscularity. Perhaps this late Victorian ideal of manhood was reflected in, and perhaps stimulated by, a growing militancy in Europe.(30)
Conclusion
<41>Elizabeth Grosz argues that a person with an abnormal body (a “freak”) “is an ambiguous being whose existence imperils categories and oppositions dominant in social life” (57). Rosemarie Garland Thomson suggests that “corporeal ambiguity is culturally intolerable [. . .] because it questions the integrity of received images of the human self” (14). I would say that the particular case of corporeal ambiguity examined here—precocious puberty—was intolerable because it brought disorder into the received structures of the gendered development of male and female bodies and endangered the received relations of adults and children. With respect to females in early puberty, the doctors found a resolution in the elision of the difference between precocious female children and adult women. Both should be docile, modest, submissive. Both might be objects of desire.
<42>Early male puberty was, by contrast, particularly disruptive of the norms in the relations of men and boys. While adult females could, in many contexts, be seen as little more than large children, the norms of chronological evolution (as well as race and class) set the standards for man-boy relations—the man’s power and the boy’s subjection. The boy with early puberty confounded this relationship with his extraordinary musculature, strength, and sexual precocity. At the same time that he was childish, undisciplined, wrathful, and weeping, he also threatened to disrupt the male social order.